Short Answer
POTS — postural orthostatic tachycardia — is a chronic problem with how your body handles standing. When you stand, your heart rate rises too much and stays high, and you may feel lightheaded, shaky, foggy, exhausted, nauseated, or aware of a pounding heartbeat. It is one form of dysautonomia, meaning a disorder of the autonomic nervous system — the system that helps regulate heart rate, blood pressure, sweating, digestion, and temperature without conscious effort. Johns Hopkins describes POTS as a blood-circulation disorder marked by symptoms when upright plus an exaggerated heart-rate rise during standing or tilt testing. (hopkinsmedicine.org)
POTS is often discussed next to vasovagal syncope because both can involve dizziness, near-fainting, fainting, heat sensitivity, standing intolerance, and autonomic reflexes. But they are not the same. In POTS, the defining pattern is tachycardia on standing without the blood-pressure drop that defines orthostatic hypotension. In vasovagal syncope, the defining event is a reflex faint, usually from a sudden fall in blood pressure and/or heart rate. (sciencedirect.com)
POTS is a “heart problem” mostly in name. The heart is often structurally normal; the problem is usually how blood vessels, blood volume, venous return, and autonomic signals respond to gravity. Johns Hopkins notes that “in most patients with POTS, the structure of the heart itself is normal,” while symptoms can come from low circulating volume, blood pooling below the heart, and stress-hormone signaling when upright. (hopkinsmedicine.org)
POTS at a glance
What is it? — Excessive heart-rate rise on standing, with orthostatic symptoms, and without a major blood-pressure drop. (sciencedirect.com)
What family? — Dysautonomia — a disorder of the autonomic nervous system. (hopkinsmedicine.org)
Is the heart diseased? — Usually no. Many people with POTS have a structurally normal heart; the issue is often circulation and autonomic control on standing. (hopkinsmedicine.org)
Who gets it? — POTS is more common in women and often affects people from adolescence through midlife; NINDS says it mainly affects people ages 15–50. (ninds.nih.gov)
Diagnosed how? — A sustained heart-rate rise of at least 30 bpm in adults, or at least 40 bpm in adolescents, within the first 10 minutes of standing or head-up tilt, with orthostatic hypotension ruled out. (sciencedirect.com)
Related faint? — Vasovagal syncope is related but different: it is a reflex faint with sudden blood-pressure and/or heart-rate drop. (my.clevelandclinic.org)
Cure? — There is no single cure, but many people improve with layered management: fluids, salt when appropriate, compression, exercise/rehab, trigger planning, and sometimes medication. (my.clevelandclinic.org)
What is POTS?
When you stand up, gravity pulls blood toward your legs, pelvis, and abdomen. Your body is supposed to respond quickly: blood vessels tighten, the heart rate rises modestly, and enough blood keeps returning to the heart and brain. In POTS, that adjustment does not coordinate well. The heart may race because the body is trying to maintain blood flow while upright. Cleveland Clinic describes this as a failure to coordinate blood-vessel constriction and heart-rate response during position change. (my.clevelandclinic.org)
The clinical threshold most often used is a sustained heart-rate rise of at least 30 beats per minute in adults within 10 minutes of standing or head-up tilt. For adolescents, the threshold is at least 40 beats per minute. The diagnosis also requires that orthostatic hypotension is not the explanation; orthostatic hypotension is usually defined as a systolic blood-pressure fall of at least 20 mmHg or a diastolic fall of at least 10 mmHg within 3 minutes of standing. (sciencedirect.com)
POTS "is defined by chronic orthostatic intolerance accompanied by an excessive increment in sinus heart rate on standing in the absence of significant orthostatic hypotension" (10.3389/fneur.2026.1806502).
This is why “heart problem POTS” can be a misleading phrase. Tachycardia POTS does involve a fast heart rate, but the fast rate is often the visible sign of a broader POTS orthostatic problem: venous pooling, low effective circulating volume, autonomic signaling, deconditioning, small-fiber/autonomic nerve involvement in some people, or overlapping conditions that affect circulation. Johns Hopkins lists lower circulating blood volume, excessive pooling below the heart when upright, and elevated epinephrine/norepinephrine signaling as contributors in many patients. (hopkinsmedicine.org)
The body mechanics in plain English
Gravity pulls blood downward. — Blood may pool too much below the heart. (hopkinsmedicine.org)
Blood vessels squeeze to push blood back upward. — Vessels may not tighten efficiently. (hopkinsmedicine.org)
Heart rate rises a little. — Heart rate rises excessively and stays high. (sciencedirect.com)
Brain blood flow is protected. — You may feel lightheaded, foggy, weak, shaky, nauseated, or close to fainting. (hopkinsmedicine.org)
Dysautonomia — the umbrella POTS sits under
POTS is "postural tachycardia syndrome (POTS), a form of dysautonomia" (PMID 41528744).
Dysautonomia means the autonomic nervous system is not regulating automatic body functions normally. “Autonomic” refers to functions you do not consciously control: heart rate, blood pressure, sweating, digestion, pupil size, and temperature regulation. Johns Hopkins describes POTS as a form of dysautonomia, and Cleveland Clinic lists POTS and vasovagal syncope among dysautonomia-related conditions. (hopkinsmedicine.org)
People also search for autonomic dysfunction or autonomic dysautonomia. In patient language, these terms point to the same neighborhood: the body’s autopilot is struggling to adjust to position, heat, meals, exertion, stress, hydration, or illness. POTS is one named pattern inside that neighborhood; it is not the only one. Orthostatic hypotension, vasovagal syncope, inappropriate sinus tachycardia, and some neuropathies can also involve autonomic regulation. (ncbi.nlm.nih.gov)
POTS vs vasovagal syncope vs orthostatic hypotension
| | POTS | Vasovagal syncope | Orthostatic hypotension |
|---|---|---|---|
| Core sign | Heart rate rises excessively on standing: at least 30 bpm in adults or at least 40 bpm in adolescents within 10 minutes, without orthostatic hypotension. (sciencedirect.com) | Reflex faint: blood pressure and/or heart rate drop suddenly, reducing blood flow to the brain. (my.clevelandclinic.org) | Blood pressure drops on standing: at least 20 mmHg systolic or 10 mmHg diastolic within 3 minutes. (ncbi.nlm.nih.gov) |
| Main experience | Upright intolerance: racing heart, lightheadedness, palpitations, brain fog, fatigue, tremor, nausea, exercise intolerance. (hopkinsmedicine.org) | Fainting or near-fainting, often with warmth, nausea, sweating, pallor, tunnel vision, or a slow pulse beforehand. (my.clevelandclinic.org) | Dizziness, blurred vision, syncope, or other symptoms from low blood pressure after standing. (ncbi.nlm.nih.gov) |
| Faints? | Can happen, but fainting is not required for POTS. (hopkinsmedicine.org) | Fainting is the defining event. (my.clevelandclinic.org) | Can faint if blood pressure drops enough. (ncbi.nlm.nih.gov) |
| Common triggers | Standing, heat, dehydration, skipped meals, illness, prolonged upright time, sometimes post-viral onset. (hopkinsmedicine.org) | Needles, blood, pain, emotional stress, exhaustion, standing too long, heat. (my.clevelandclinic.org) | Standing up, medications, dehydration, neurologic disease, diabetes, and other causes depending on the person. (pubmed.ncbi.nlm.nih.gov) |
| Overlap | May share fluids, salt when appropriate, compression, and graded exercise/rehab strategies. (hopkinsmedicine.org) | May share trigger education, hydration, compression, and counter-pressure maneuvers. (my.clevelandclinic.org) | Management differs because the primary abnormality is blood-pressure fall, not isolated orthostatic tachycardia. (pubmed.ncbi.nlm.nih.gov) |
The simplest way to remember it
POTS: “My heart races when I’m upright, and symptoms improve when I lie down.”
Vasovagal syncope: “A reflex makes my blood pressure and/or heart rate drop, and I faint.”
Orthostatic hypotension: “My blood pressure drops when I stand.”
These can overlap in real life. A person with POTS can also have fainting episodes. A person with vasovagal syncope can also feel awful with prolonged standing. That is one reason evaluation matters: the treatment plan depends on which pattern is actually present. (sciencedirect.com)
Who gets POTS, and why
POTS "is a chronic form of orthostatic intolerance that primarily affects female patients" (10.1111/joim.70104).
NINDS says POTS mainly affects people ages 15–50 and is more common in women than men. A Journal of Internal Medicine review reports that POTS affects younger individuals ages 15–45, has a distinct female predominance of about 80%, and estimates prevalence in developed countries at 0.2%–1.0%. Johns Hopkins and Cleveland Clinic both describe U.S. prevalence as commonly estimated at 1–3 million people. (ninds.nih.gov)
In a 2026 single-center case-control study of 305 patients with POTS, 264 met criteria for central sensitization syndrome; among those, 234 were female, reported as 88.6% of the central-sensitization group, and 264/305, or 86.6%, met the study’s central-sensitization criteria. This does not mean all POTS is pain-related or anxiety-related. It means that in that referred clinical cohort, pain-processing, sensory symptoms, anxiety/depression burden, headaches, IBS, and related symptoms were common enough to deserve careful clinical attention rather than dismissal. (pubmed.ncbi.nlm.nih.gov)
POTS often begins or worsens after a physiologic stressor. NINDS lists pregnancy, major surgery, puberty, trauma, or viral illness as common onset contexts. Cleveland Clinic similarly lists significant illness, pregnancy, physical trauma, and surgery as higher-risk contexts. A 2019 review also describes onset after immunologic or physiologic stressors such as viral infection, vaccination, trauma, pregnancy, surgery, or psychosocial stress. (ninds.nih.gov)
Common “why me?” patterns clinicians may look for
Post-viral or post-infectious onset — POTS can begin after viral illness; Long COVID and ME/CFS research has increased attention to orthostatic intolerance and dysautonomia. (ninds.nih.gov)
Hypermobility or hEDS — NINDS notes that some people with hypermobile Ehlers-Danlos syndrome may also be diagnosed with POTS. (ninds.nih.gov)
Migraine, IBS, fatigue syndromes — NINDS lists migraine, IBS, ME/CFS, and Long COVID among conditions associated with POTS. (ninds.nih.gov)
Autoimmune or connective-tissue conditions — Cleveland Clinic notes higher likelihood in people with autoimmune conditions such as Sjögren’s syndrome, lupus, and celiac disease. (my.clevelandclinic.org)
Deconditioning after bed rest or reduced activity — POTS symptoms can make activity harder, and reduced activity can worsen orthostatic tolerance, so rehab often starts gently and may begin recumbent. (hopkinsmedicine.org)
Vasovagal syncope — the big overlapping topic
Vasovagal syncope is the classic “common faint.” Cleveland Clinic describes it as a nervous-system overreaction that makes blood pressure and heart rate drop suddenly, causing fainting; Johns Hopkins calls reflex syncope the most frequent cause of fainting. (my.clevelandclinic.org)
A vasovagal response often has a warning phase. People may feel suddenly warm, nauseated, sweaty, pale, lightheaded, yawny, or notice tunnel vision. Triggers can include needles, seeing blood, pain, emotional stress, exhaustion, or standing too long. (my.clevelandclinic.org)
The overlap with POTS is practical: both conditions can be worse with heat, dehydration, and prolonged upright posture; both may improve with thoughtful hydration, trigger planning, and compression in selected people. The difference is the physiology. In POTS, the main measurable sign is excessive orthostatic tachycardia. In vasovagal syncope fainting, the event is a reflex drop in blood pressure and/or heart rate that briefly reduces brain blood flow enough to pass out. (sciencedirect.com)
What to do when a vasovagal episode may be starting
If you have a known vasovagal pattern and feel the prodrome, the safest first step is usually to sit or lie down before you fall. Counter-pressure maneuvers — such as leg crossing with muscle tensing, handgrip, or arm tensing — can raise blood pressure in some people during the warning phase; a 2022 review found symptom improvement with counter-pressure maneuvers in laboratory and community settings, while noting practical limits such as needing to recognize the faint early. (my.clevelandclinic.org)
Compression can also be part of the plan. Cleveland Clinic notes that waist-high medical-grade compression stockings may help vasovagal syncope, and Johns Hopkins notes that compression garments may reduce excessive blood pooling in POTS. For POTS, many clinicians prefer higher-coverage garments — waist-high or abdominal-plus-leg compression — because pooling is not only in the calves. Discuss the right compression level and garment type with your clinician, especially if you have vascular disease, neuropathy, skin breakdown, or clotting history. (my.clevelandclinic.org)
Conditions that travel with POTS
POTS does not always travel alone. Some people have one clean orthostatic problem; others have a cluster of symptoms across pain, digestion, migraine, fatigue, allergic-type symptoms, pelvic symptoms, or hypermobility. The point is not to self-diagnose every associated condition. The point is to recognize patterns that are worth bringing to a clinician.
POTS overlaps with post-viral illness: a 2026 study describes "dysautonomia with orthostatic intolerance" (PMID 41576003) as a shared feature of Long COVID and ME/CFS.
A 2026 study comparing Long COVID and ME/CFS describes overlapping features including post-infectious onset, brain fog, fatigue, muscle pain, and dysautonomia with orthostatic intolerance. NINDS also lists ME/CFS, Long COVID, migraine, IBS, traumatic brain injury, and hEDS among conditions associated with POTS. (pmc.ncbi.nlm.nih.gov)
POTS/orthostatic intolerance has also been studied alongside pelvic venous disorders. A 2026 PMC article reports two retrospective studies assessing POTS or POTS-like orthostatic intolerance with pelvic venous disorders and symptom change after iliac vein stenting. This is an emerging area, not a reason to assume pelvic venous disease is the cause of your symptoms. It is a reason to tell your clinician if orthostatic symptoms coexist with pelvic heaviness/pain, leg swelling, urinary symptoms, or menstrual-related symptom patterns. (pmc.ncbi.nlm.nih.gov)
Ask a clinician about overlapping conditions when you notice:
Joint hypermobility, frequent sprains, stretchy skin, chronic joint pain — POTS can coexist with hypermobility disorders, including hEDS. (ninds.nih.gov)
Flushing, hives, food reactions, wheezing, “allergic” flares — Some POTS patients report mast-cell-type symptoms; evaluation should be individualized because symptoms can have many causes. (hopkinsmedicine.org)
Migraine, severe headaches, light sensitivity — Migraine is listed among conditions associated with POTS. (ninds.nih.gov)
GI dysmotility, nausea, IBS-like symptoms — NINDS lists digestive issues and IBS among POTS symptoms/associated conditions. (ninds.nih.gov)
Long COVID or ME/CFS symptoms with standing intolerance — Long COVID and ME/CFS research describes dysautonomia and orthostatic intolerance overlap. (pmc.ncbi.nlm.nih.gov)
Pelvic heaviness, pelvic pain, leg swelling, urinary symptoms — Pelvic venous disorders are being studied in POTS/OI populations; this needs clinician evaluation, not self-treatment. (pmc.ncbi.nlm.nih.gov)
How POTS is diagnosed and managed, in brief
POTS diagnosis usually starts with a careful history, medication review, physical exam, and orthostatic vital signs. The key test is often a 10-minute standing test or head-up tilt-table test, with heart rate and blood pressure measured over time. Johns Hopkins says POTS is diagnosed with a 10-minute standing test or tilt-table test, and that other tests may be used to identify specific features in some patients. (hopkinsmedicine.org)
A clinician also has to rule out other reasons for tachycardia or dizziness: dehydration, blood loss, anemia, thyroid disease, infection, medication effects, arrhythmias, pregnancy-related issues, and orthostatic hypotension. POTS is not diagnosed just because a wearable shows a high heart rate when you stand. The pattern, symptoms, duration, blood pressure, context, and exclusions all matter. (sciencedirect.com)
Management is layered. Most plans begin with non-drug strategies: fluids, salt if appropriate for your blood pressure/kidney/heart situation, compression garments, sleep and trigger planning, and graded exercise or physical therapy that may start recumbent or semi-recumbent. Medication may be considered when symptoms remain frequent or disabling, but there is no single medication that works for everyone. (hopkinsmedicine.org)
When to see a doctor
Get medical evaluation for new, persistent, worsening, or unexplained dizziness, fainting, racing heart, chest symptoms, or exercise intolerance. POTS and vasovagal syncope can be manageable, but similar symptoms can come from anemia, dehydration, thyroid disease, arrhythmias, structural heart disease, medication effects, neurologic conditions, pregnancy-related complications, or blood-pressure disorders. (pubmed.ncbi.nlm.nih.gov)
Seek urgent care or emergency evaluation if you faint during exertion, faint while lying down, have chest pain, severe shortness of breath, a new irregular heartbeat, neurologic symptoms, serious injury from a fall, black or bloody stools, severe dehydration, or a first-ever fainting episode without a clear benign trigger. Cleveland Clinic advises emergency medical care after passing out because serious or life-threatening conditions can cause syncope. (my.clevelandclinic.org)
How Welltory fits
A wearable and the Welltory Science Lab Orthostatic Test can help you track how your heart rate changes from lying or sitting to standing, how long the rise lasts, and how symptoms line up with sleep, stress, illness, hydration, heat, meals, menstrual cycle, and exercise. That kind of trend can make a clinician conversation more concrete.
Welltory does not diagnose POTS, vasovagal syncope, orthostatic hypotension, dysautonomia, arrhythmia, or any other medical condition. Think of it as a structured tracking tool: useful for patterns, not a substitute for a clinician’s exam, orthostatic vitals, ECG when needed, blood work, or tilt/stand testing.
What our own data shows
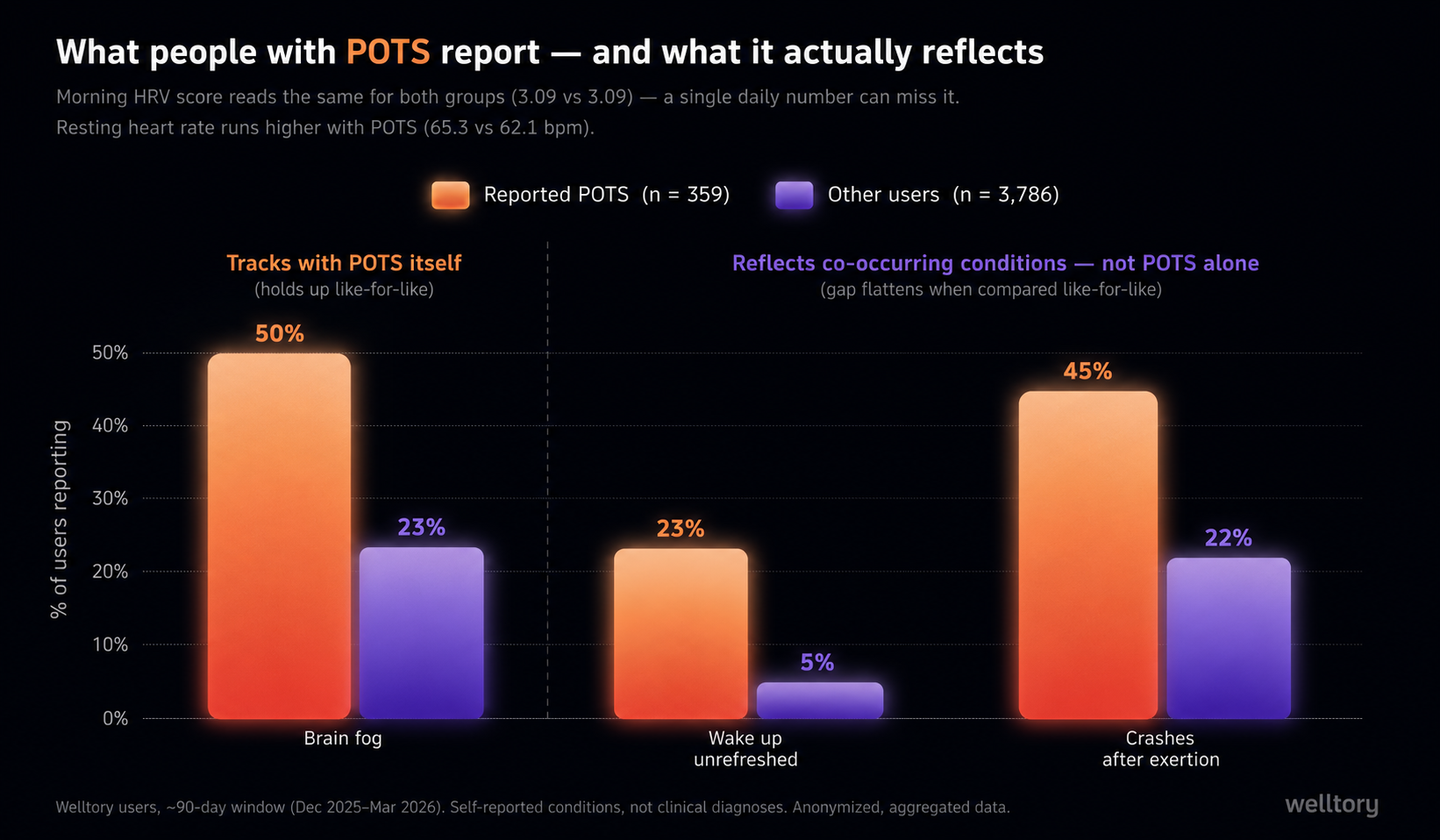
The POTS signal is in the data — but a one-number score buries it. Among 359 Welltory users who reported having POTS and also wear a tracker, the raw signal you'd expect from POTS is present: their resting heart rate runs higher than other users' (a median of 65.3 vs 62.1 bpm). And the day-to-day experience is real, not imagined — this is worth naming, because people with POTS are so often told it's "all in their head." These users report brain fog about twice as often (50% vs 23%), and that gap holds up even when we compare people carrying the same number of other conditions — so it tracks with POTS itself. They also wake up unrefreshed far more often (23% vs 5%) and report frequent post-exertion crashes about twice as often (45% vs 22%); these two are just as real to live with, but on a closer look they appear to reflect the whole cluster of conditions that tend to travel with POTS — like ME/CFS, Long COVID, or migraine — rather than POTS on its own. What almost none of this surfaces in is the single morning HRV *score most people glance at: it reads statistically identical to everyone else's (3.09 vs 3.09*), and morning energy and sleep scores read about the same.
So the tracker isn't blind — the POTS signal is already in the underlying data, like resting heart rate. What a single combined daily number can't do is carry it. For POTS, the useful information lives in the right slice of the data you already have, not in one summary score.
How we know this: these figures compare an in-app survey (which conditions people have and how they feel) with wearable-derived morning scores, for 359 Welltory users who reported POTS and tracked over a roughly 90-day window (December 2025–March 2026), against 3,786 users without POTS who had the same data (~68% US). We also looked like-for-like: we split users by how many other conditions they report and compared POTS vs non-POTS within each group. The brain-fog gap held up across those groups, so we attribute it to POTS itself; the waking-unrefreshed and post-exertion-crash gaps mostly flattened out within groups, which is why we describe those two as reflecting the co-occurring conditions rather than POTS alone. The morning HRV figure is Welltory's transformed HRV score, not raw RMSSD in milliseconds; with this sample size a real difference would be detectable, so the non-difference means "no difference in this score," not a scale limit. These are self-reported conditions, not clinical diagnoses, from a self-selected group of users; we also checked that this isn't simply milder cases who kept tracking. All figures are reported as anonymized, aggregated data; no individual user is identifiable.
The numbers behind this
| What we compared | POTS (n = 359) | Other users (n = 3,786) | What it means |
|---|---|---|---|
| Brain fog | 50% | 23% | Holds up comparing like-for-like → tracks with POTS itself |
| Wake up unrefreshed | 23% | 5% | Real and common — but reflects the co-occurring conditions, not POTS alone |
| Frequent crashes after exertion | 45% | 22% | Real and common — but reflects the co-occurring conditions, not POTS alone |
| Resting heart rate (median) | 65.3 bpm | 62.1 bpm | Objective POTS-linked signal a single daily score hides |
| Morning HRV score (median) | 3.09 | 3.09 — no measurable difference | The one-number score doesn't carry the POTS signal |
| Sleep score (median) | 0.97 | 0.98 | Essentially the same |
Based on self-reported POTS among 12,387 surveyed Welltory users (~68% US), 2025–2026; figures are reproducible from our own data. Limitations: conditions and symptoms are self-reported (not clinical diagnoses) from a self-selected group of users; we verified the result is not an artifact of only milder users staying in tracking, and that the brain-fog gap persists after accounting for the number of co-occurring conditions.
How we made it
Made with AI tools, then edited, fact-checked, and medically reviewed by the Welltory team. See our [Editorial & AI Policy].
Discounts for blog readers: up to 36% off
See what affects your energy, stress, sleep, and daily state with Welltory
This is general education about POTS and related conditions. It does not diagnose you. A fast heart rate, fainting, or dizziness on standing can have many causes, so any new or persistent symptoms should be checked by a qualified clinician.
Was this helpful?
Ask AI for a summary of page
Written by Jane Smorodnikova

The founder and CEO of Welltory. A recognized tech leader with two Master's degrees and experience at MIT, she has scaled Welltory to over 17 million users.
Written by Kseniia Iaroslavtseva

She reviews scientific research and turns it into structured, readable insights.
Reviewed by Anna Elitzur
-2.jpg)
With her medical degree, Anna reviews Welltory's health content for medical accuracy and alignment with current clinical guidelines and research.
References
- 2015 Heart Rhythm Society Expert Consensus Statement on the diagnosis and treatment of postural tachycardia syndrome, inappropriate sinus tachycardia, and vasovagal syncope. https://www.sciencedirect.com/science/article/pii/S1547527115003288
- National Institute of Neurological Disorders and Stroke: Postural Tachycardia Syndrome (POTS). https://www.ninds.nih.gov/health-information/disorders/postural-tachycardia-syndrome-pots
- Johns Hopkins Medicine: Postural Orthostatic Tachycardia Syndrome (POTS). https://www.hopkinsmedicine.org/health/conditions-and-diseases/postural-orthostatic-tachycardia-syndrome-pots
- Cleveland Clinic: Postural Orthostatic Tachycardia Syndrome (POTS). https://my.clevelandclinic.org/health/diseases/16560-postural-orthostatic-tachycardia-syndrome-pots
- Cleveland Clinic: Vasovagal Syncope. https://my.clevelandclinic.org/health/symptoms/23325-vasovagal-syncope
- Johns Hopkins Medicine: Syncope (Fainting). https://www.hopkinsmedicine.org/health/conditions-and-diseases/syncope-fainting
- NCBI MeSH: Orthostatic Hypotension definition. https://www.ncbi.nlm.nih.gov/mesh/68007024
- Fedorowski A. Postural orthostatic tachycardia syndrome: clinical presentation, aetiology and management. Journal of Internal Medicine. https://pubmed.ncbi.nlm.nih.gov/30372565/
- Prevalence of Central Sensitization in Postural Tachycardia Syndrome. JAMA Network Open / PubMed. https://pubmed.ncbi.nlm.nih.gov/41528744/
- Shared autonomic phenotype of long COVID and myalgic encephalomyelitis/chronic fatigue syndrome. https://pmc.ncbi.nlm.nih.gov/articles/PMC12829881/
- Orthostatic Challenge Causes Distinctive Symptomatic, Hemodynamic and Cognitive Responses in Long COVID and ME/CFS. https://pmc.ncbi.nlm.nih.gov/articles/PMC9285104/
- Association and post-iliac vein stenting symptom improvement of POTS/OI with pelvic venous disorders. https://pmc.ncbi.nlm.nih.gov/articles/PMC12887661/
- Counter pressure maneuvers for syncope prevention: semi-systematic review and meta-analysis. https://pmc.ncbi.nlm.nih.gov/articles/PMC9606335/
- Harvard Health: POTS overview and diagnosis/treatment coverage. https://www.health.harvard.edu/diseases-and-conditions/hit-hard-by-pots


